

What is a ‘Silo’ in MSK?
What is a ‘Silo’ in MSK?
Understanding silo based learning in musculoskeletal practice
Understanding silo based learning in musculoskeletal practice

What is a ‘Silo’ in MSK?
Understanding silo based learning in musculoskeletal practice
What Is a Silo — And Why Does Silo-Based Working Hold Back Injured Patients and Athletes?
8 minutes read - to change your clinical reasoning
In MSK healthcare, we often talk about the importance of “joined-up care”, “multidisciplinary working” and “seeing the full picture”.
But the reality is this:
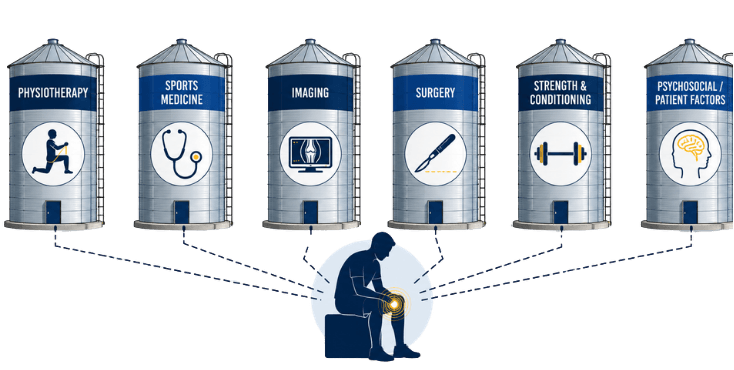
Many injured patients and athletes are still managed in silos.
A physiotherapist looks at movement.
A doctor looks at diagnosis.
A radiologist looks at imaging.
A strength and conditioning coach looks at performance.
A surgeon looks at structural pathology.
A psychologist may look at confidence, fear or readiness.
Each professional may be doing good work.
But if those views are not connected, the patient can be left with fragmented care, mixed messages and unclear direction.
That is where silo-based working becomes a problem.
What Is a Silo?
A silo is when information, knowledge or decision-making sits separately from everything else.
In healthcare, this often means different professionals, departments or areas of expertise working in isolation rather than connecting their thinking.
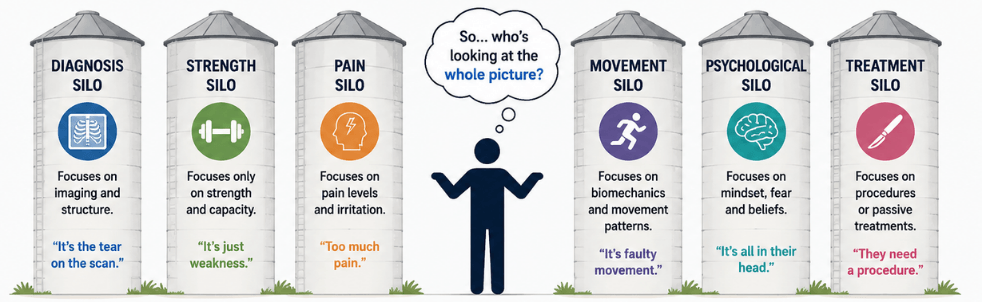
In MSK practice, a silo might look like this:
A clinician focuses only on the MRI scan.
Another focuses only on strength testing.
Another focuses only on pain.
Another focuses only on biomechanics.
Another focuses only on return to sport timelines.
The issue is not that any of these areas are wrong.
The issue is when they are viewed separately, rather than being integrated into one clear clinical picture.
Why Does This Matter in Injury Management?
Injured patients and athletes are rarely simple.
Pain is not just tissue damage.
Imaging is not always the full answer.
Strength is not the same as confidence.
A diagnosis does not automatically tell us the best treatment plan.
A return-to-sport test does not always tell us whether someone is truly ready.
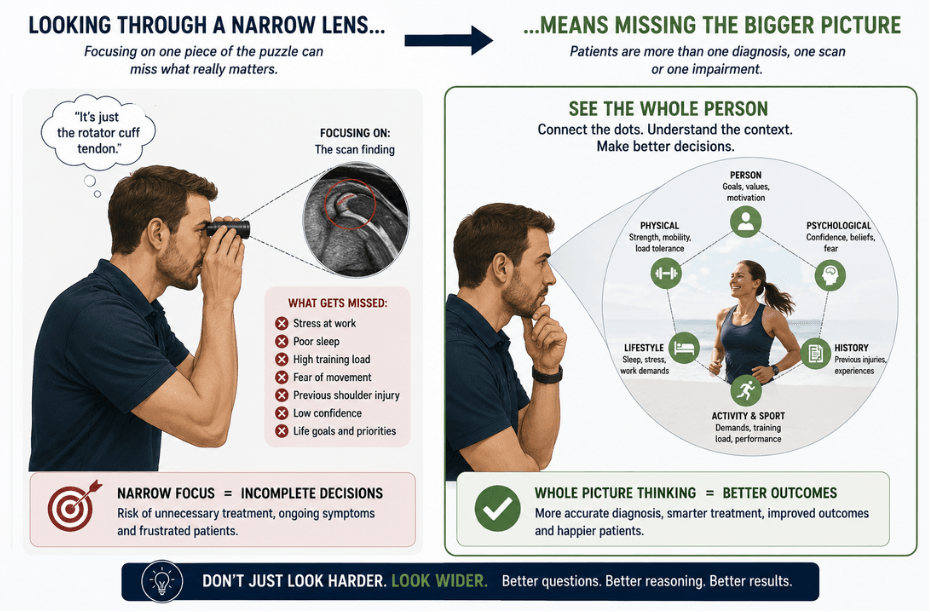
When we manage patients through one narrow lens, we risk missing the bigger picture.
For example, a patient with a meniscal tear may have an MRI-confirmed structural finding, but that does not automatically mean surgery is the right next step.
We also need to consider:
Their mechanism of injury.
Their symptom behaviour.
Their load tolerance.
Their goals.
Their confidence.
Their sport or work demands.
Their previous history.
Their expectations.
Their response to rehabilitation.
Their risk factors.
Their understanding of the problem.
Without this wider reasoning process, management can become too simplistic.
The Problem With Silo-Based Working
Silo-based working can lead to several common problems in MSK care.
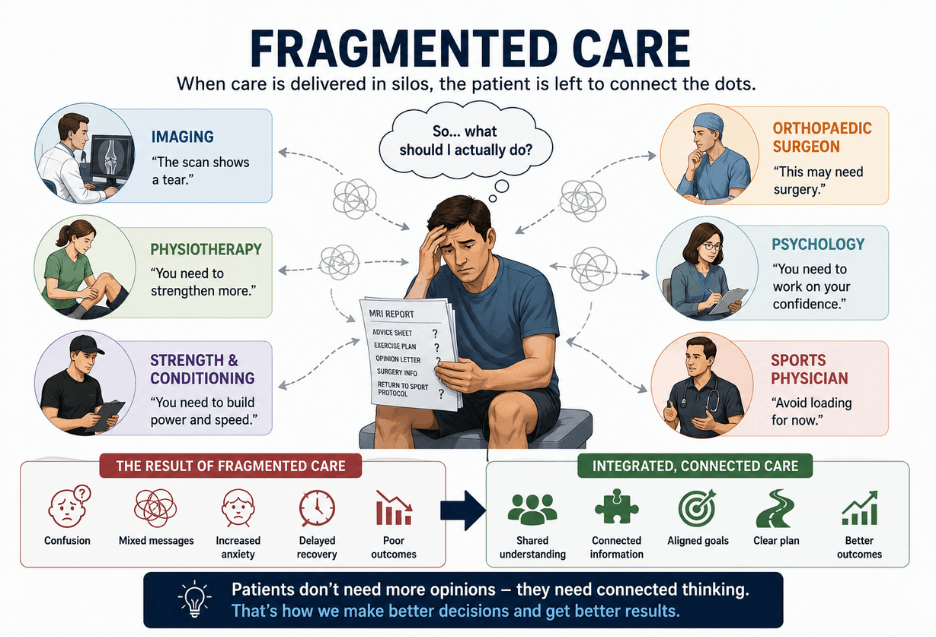
1. Patients receive mixed messages
One professional may say, “Your scan shows damage.”
Another may say, “You just need strengthening.”
Another may say, “Avoid impact.”
Another may say, “You can return when pain settles.”
The patient is then left confused.
They may not know who to trust, what to do next, or what their injury actually means.
This can increase anxiety, reduce confidence and make decision-making harder.
2. Treatment becomes too diagnosis-led
Diagnosis matters.
But diagnosis alone does not tell us everything.
Two patients can have the same diagnosis but need completely different management plans.
One person with an ACL injury may need surgical reconstruction due to instability, pivoting sport demands and performance goals.
Another may manage well with high-quality rehabilitation, good strength recovery and no functional instability.
The diagnosis is important, but the reasoning behind the decision is what matters most.
3. Imaging can become overvalued
Imaging is incredibly useful when used well.
But scans need context.
An MRI finding does not always explain pain.
Structural change does not always equal poor function.
A visible abnormality does not always mean it is the dominant driver of symptoms.
When imaging is interpreted in isolation, patients may become fearful of their body.
They may start to believe they are damaged, fragile or unsafe to move.
Good clinical reasoning helps us explain imaging in a way that is accurate, balanced and useful.
4. Rehabilitation can become too protocol-driven
Protocols can be helpful.
But patients are not protocols.
A time-based plan may say someone should be running at a certain week, jumping at another week and returning to sport by a certain month.
But clinical reality is rarely that neat.
Progression should consider tissue healing, strength, movement quality, symptoms, confidence, capacity, sport demands and risk.
If we only follow a protocol without reasoning, we may progress someone too quickly, hold them back unnecessarily, or miss the real reason they are struggling.
5. The patient’s goals can get lost
A recreational runner, a professional footballer, a manual worker and a parent wanting to play with their children may all present with a knee injury.
But their goals, pressures, risks and priorities may be completely different.
Silo-based working can sometimes focus too heavily on the injury and not enough on the person.
Good MSK care should ask:
What matters to this person?
What are they trying to get back to?
What are they worried about?
What decisions do they need to make?
What does success look like for them?
Why Silo-Based Working Is Not Effective for Injured Athletes
Athletes are a perfect example of why silo-based care falls short.
An athlete does not just need pain relief.
They need a plan that connects:
Diagnosis
Tissue healing
Strength
Power
Speed
Movement quality
Training load
Psychological readiness
Sport-specific demands
Risk management
Communication with coaches
Return-to-performance planning

If these areas are not connected, return to sport can become unsafe, delayed or poorly planned.
An athlete may be physically strong but psychologically unready.
They may pass gym-based tests but fail under fatigue.
They may have good range of movement but poor change-of-direction control.
They may be pain-free but not prepared for the chaos of sport.
This is why clinical reasoning needs to move beyond isolated thinking.
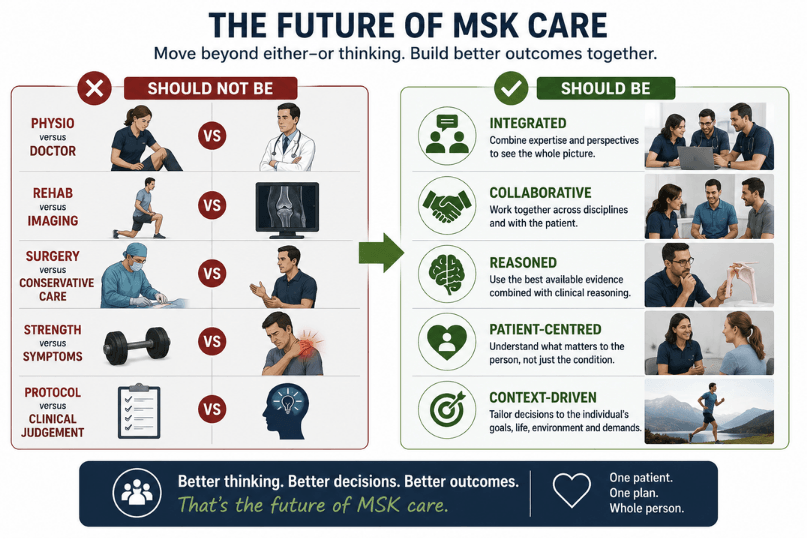
The Better Approach: Clinical Reasoning Without Silos
At Simply MSK, we believe the best clinical decisions happen when information is connected.
Not when each professional stays in their own lane and protects their own viewpoint.
But when clinicians can step back and ask:
What is the full clinical picture?
Which information matters most?
What is the dominant driver?
What risks need considering?
What does this patient need right now?
What decision is most appropriate, and why?
This is the foundation of Clinical Reasoning Without Silos.
It is not about replacing specialist knowledge.
It is about connecting specialist knowledge.
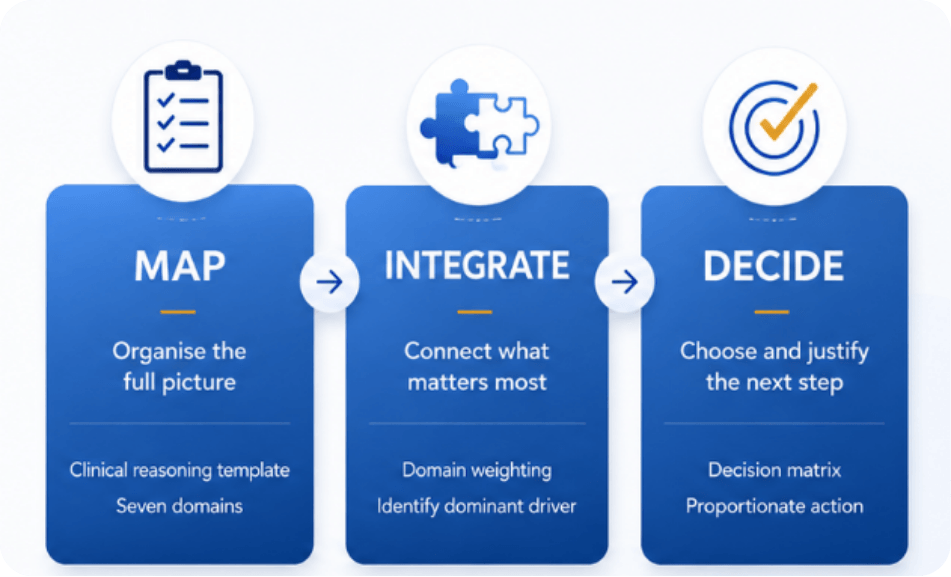
The Simply MSK approach is built around a structured reasoning model: Seven Clinical Reasoning Domains and a repeatable process that moves from clinical problem, to information gathering, to domain weighting, to dominant driver, to decision-making and clinical action.
What Does This Look Like in Practice?
Instead of asking:
“What structure is injured?”
We also ask:
Why has this happened?
How is it behaving?
What can the patient currently tolerate?
What are they afraid of?
What do they believe is wrong?
What does the imaging actually mean?
What are the risks?
What is the best next decision?
This creates a much more complete picture.
It helps clinicians move away from isolated assessment findings and towards integrated decision-making.
That is where confidence grows.
For both the clinician and the patient.
Why This Matters for Less Experienced Clinicians
For students, junior clinicians and clinicians developing in MSK, silo-based learning is incredibly common.
You may learn anatomy in one place.
Special tests in another.
Rehab exercises somewhere else.
Imaging on a separate course.
Psychosocial factors in another module.
Return to sport as another topic entirely.
But real patients do not present in neat categories.
They present with messy, overlapping information.
That is why many clinicians can know a lot of individual facts but still feel unsure when making decisions.
Clinical reasoning is the skill that connects the information together.
Without it, MSK practice can feel overwhelming.
With it, assessment, treatment planning and decision-making become much clearer.

Moving Beyond Silo-Based Care
Silo-based working is not ineffective because specialists are unhelpful.
It is ineffective because patients need connected thinking.
Silo-based working is not ineffective because specialists are unhelpful.
It is ineffective because patients need connected thinking.
Want to Improve Your Clinical Reasoning?
If you are an MSK clinician, student, therapist or healthcare professional who wants to feel more confident managing injured patients, our Clinical Reasoning Without Silos Framework is designed to help.
It gives you a clear structure to move beyond isolated assessment findings and start connecting the full clinical picture.
The Simply MSK model is built around a fixed set of clinical reasoning domains and a repeatable reasoning process, helping clinicians move from the clinical problem, to information gathering, to domain weighting, to identifying the dominant driver, to making a justified clinical decision.
You will learn how to think through:
Mechanism and context
Symptom behaviour
Load tolerance and capacity
Expectations and psychosocial factors
Red flags and risk
Imaging and investigations
Clinical decisions
So you can stop relying on isolated pieces of information and start making clearer, more confident, patient-centred decisions.
Download the Clinical Reasoning Without Silos Framework and start building a more connected way to think, reason and manage MSK patients.
References
Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. Journal of Bone and Joint Surgery American Volume. 1995;77(1):10-15.
Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. Journal of Shoulder and Elbow Surgery. 1999;8(4):296-299.
Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. American Journal of Sports Medicine. 1998;26(3):360-366.
Mellor R, Bennell K, Grimaldi A, et al. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. BMJ. 2018;361:k1662.
Beard DJ, Rees JL, Cook JA, et al. Arthroscopic subacromial decompression for subacromial shoulder pain: a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial. The Lancet. 2018;391(10118):329-338.
Paavola M, Malmivaara A, Taimela S, et al. Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: randomised, placebo surgery controlled clinical trial. BMJ. 2018;362:k2860.
Griffin DR, Dickenson EJ, Wall PDH, et al. Hip arthroscopy versus best conservative care for the treatment of femoroacetabular impingement syndrome: UK FASHIoN multicentre randomised controlled trial. The Lancet. 2018;391(10136):2225-2235.
Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. Annals of Family Medicine. 2013;11(6):527-534.
Ardern CL, Österberg A, Tagesson S, Gauffin H, Webster KE, Kvist J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. British Journal of Sports Medicine. 2014;48(22):1613-1619.
Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British Journal of Sports Medicine. 2016;50(13):804-808.

Multidisciplinary MSK education built by clinicians, for clinicians.
Designed to improve real-world decision-making.
Trusted by 500+ MSK Clinicians Across The UK

Learn
Simply MSK LTD © 2026 14720655, registered in England and Wales All rights reserved




Subscribe here for free
We HATE spam. Your email address is 100% secure